It is general knowledge that, as we age, our sensory systems start to decline. This includes sight, smell, temperature regulation and balance mechanisms. It’s important to have good balance because if it declines, you are at a higher risk for falling. And falling, results in injuries that can greatly affect your life.
Exercises that Challenge your Balance
What many people don’t know, is that you can work on making your balance stronger, just like you do a muscle: by exercising it! What physical therapy aims to do, is find exercises that challenge your balance system, so that your body must learn to adapt to certain situations and re-train itself on what to do.
Static and Dynamic Exercises
Physical Therapists can provide both static and dynamic exercises for you, depending on what is most challenging. Exercises can be very simple and integrated during daily routines- like balancing on one leg while brushing your teeth.
If you are having trouble with your balance, come in to Nick Rinard Physical Therapy and have an assessment by a physical therapist! 503-244-6232
More
 This is a question that seems to be in debate. At our clinic, we advise our patients to come in for treatment as soon as possible when experiencing pain in order for the fastest results. I have experienced push-back from other health care practioners who want the person to “rest” for 4-6 weeks before starting therapy. The problem with this? There are many things a person can be doing immediately after the MVA to facilitate healing and prevent dysfunction. All too often, we see people 6 months or longer after the MVA. If the patient has not been given anything to work on for exercises at home, the picture is this: limited, painful movement of the spine or joint, global weakness, and poor posture that becomes painful if corrected.
This is a question that seems to be in debate. At our clinic, we advise our patients to come in for treatment as soon as possible when experiencing pain in order for the fastest results. I have experienced push-back from other health care practioners who want the person to “rest” for 4-6 weeks before starting therapy. The problem with this? There are many things a person can be doing immediately after the MVA to facilitate healing and prevent dysfunction. All too often, we see people 6 months or longer after the MVA. If the patient has not been given anything to work on for exercises at home, the picture is this: limited, painful movement of the spine or joint, global weakness, and poor posture that becomes painful if corrected.
What does therapy look like in the first few weeks after an MVA?
- Initiate gentle range of motion exercise to prevent loss of movement
- Manual techniques including passive range of motion and soft tissue mobilization to promote blood flow and healing.
- Ultrasound modalities that decrease inflammation/swelling and promote tissue healing
- Education and training on how to prevent dysfunction
Here at Nick Rinard Physical Therapy, we see a lot of patients who have suffered an MVA. In fact, we see it so much we have a protocol for it that is very successful for treatment. Don’t wait! Start healing and feeling better today!
More
Last week, I had a patient come into the clinic with neck pain that had started the week before. He had been a patient in the past and knew that the sooner he got in for treatment, the better.
Terry had pain medial to his left shoulder blade. This pain was limiting him with sleeping and with driving, as left rotation caused pain. He was rating his pain a 4/10 at the time of the evaluation.
Evaluation and Assessment
Scapula connects Upper Arm with Collar Bone
During the evaluation, left and right rotation motions produced pain medial to the left scapula. Upon palpation, the musculature where the pain was produced was very tender, acting like trigger points. I chose not to treat the trigger points, as these things are likely secondary to the real problem: a derangement.
During the repeated movement assessment, I had Terry go through retraction, extension and flexion. When we tested repeated left rotation, Terry’s pain decreased with repetition. Terry was sent home performing repeated left rotation with over-pressure. By his next visit, his pain was significantly decreased and the trigger points of the muscles had also decreased with pain when palpated. I had Terry increase the frequency of which he was to perform the rotation exercise. By the next visit, Terry had abolition of all pain, no limitation with sleeping or driving and the trigger points were completely gone!
Getting to the Root of the Problem
The Mechanical Diagnosis and Therapy (MDT) Method is very effective at getting to the root of the problem. When the core issue is fixed, the secondary impairments almost always resolve on their own. If a clinician is always treating the symptoms and not the cause, this will lead to more visits, more time until recovery and more money from the patient. This is one of the fundamental reasons that we practice the MDT Method here at Nick Rinard Physical Therapy – to fix your core issues!
More
‘R.I.C.E.’ Coined in 1978
‘R.I.C.E.’ (rest, ice, compression, elevation) was coined in 1978 by Dr. Gabe Mirkin. Since then, ice has been the standard treatment for injuries and sore muscles. The RICE guidelines have been used for decades, but it now appears that ice and rest may delay healing.
Scientific Articles Don’t Support Ice for Healing
 A study from The American Journal of Sports Medicine, June 2013 asked athletes to exercise intensely enough to develop muscle damage that caused extensive muscle soreness. It was found that icing delayed swelling, but did not quicken the healing process. A summary of 22 scientific articles found little to no evidence supporting that ice and compression facilitate healing over compression alone.
A study from The American Journal of Sports Medicine, June 2013 asked athletes to exercise intensely enough to develop muscle damage that caused extensive muscle soreness. It was found that icing delayed swelling, but did not quicken the healing process. A summary of 22 scientific articles found little to no evidence supporting that ice and compression facilitate healing over compression alone.
Inflammation
Inflammation is required for healing. Inflammation is a part of our immune system and is essential in the healing process. Inflammatory cells migrate to the injured tissue to start the healing process. Macrophages (inflammatory cells) release a hormone into injured tissues, which helps muscles and other injured tissues heal. Applying ice to reduce swelling can delay healing by preventing the body from releasing this hormone.
Icing can also prevent healing cells from entering the injured tissues by constricting blood-flow. It can take hours for the blood vessels to return to their size. Icing can also decrease strength, speed, endurance and coordination.
General Tips for Using Ice
If you’re going to ice, only apply ice for 10-15 minutes at a time. Utilize ice for the first day of injury. Seek medical attention from a mechanical physical therapist if the pain is severe or you cannot actively move a body part.
More
 A mistake that people often make is waiting too long to start physical therapy treatment for their aches and pains. This commonly occurs because you may be thinking, “this will go away on its own,” or, “it’s just normal for me to feel like this at my age.” I want to clear up some confusion on mechanical pain versus normal muscle soreness that does not require skilled therapy or treatment.
A mistake that people often make is waiting too long to start physical therapy treatment for their aches and pains. This commonly occurs because you may be thinking, “this will go away on its own,” or, “it’s just normal for me to feel like this at my age.” I want to clear up some confusion on mechanical pain versus normal muscle soreness that does not require skilled therapy or treatment.
Muscular Pain:
- Experienced after a sudden increase in activity or exercise.
- Running 6 miles when you typically only run 2 miles
- You increased the intensity or length of time to your typical workout
- Will be experienced 1-2 days after the increased activity has been performed and will typically begin to dissipate or be gone in 3-5 days after onset.
- Is typically vague pain or experienced in a general area. The pain will not be sharp or pin-point to a specific area.
- If you’re educated on what muscles perform which actions, the sore muscles will correlate with what activity you were performing.
- Does not have increased or decreased pain associated with positions.
Mechanical Pain:
- May have a sudden onset without explanation of occurrence (you woke up with pain for no apparent reason).
- Will typically have a loss in range of motion. For example: it may be difficult to stand up straight in the morning or after prolonged sitting or driving.
- Will have positions that will increase or decrease symptoms. For example: pain increases with sitting, pain is better while lying down.
If you’re experiencing mechanical pain the sooner you seek physical therapy treatment, the better! A good Physical Therapist can determine which exercises will reduce your symptoms and get you back to doing the activities that you love!
More
A few months ago, I treated a young Portland area woman who was suffering from low back pain. “Beth” had been in a car accident 10 months prior to my evaluation. She was rating her worst pain as a 9/10 and was moderately limited with walking, sitting, bending and lifting. Because of the pain associated with these activities, Beth was limited with her duties as a student nurse, and somewhat concerned with how her back condition will affect the rest of her life. Beth had been to a chiropractor and to a different physical therapy clinic, neither of which proved to have any lasting benefits.
Beth’s objective findings included what mechanical therapists call a “Left Shift” in standing. This means that her shoulders were not centered over her hips, but rather, off to the left side. We know this as a relevant lateral component and is typically associated with a derangement (something out of alignment or out of place). Beth also demonstrated limited, painful movements of the spine; primarily in the frontal plane.
The exercise to correct Beth’s shift and reduce her derangement was repeated right side glide in standing. Beth was able to perform this exercise throughout her day to decrease her pain and by 3 weeks out, she was reporting little to no pain. Beth was then able to begin core strengthening exercises, after her pain was gone, and get back to her duties as a nursing student. At our last treatment visit, Beth told me that she was able to work multiple 12 hour shifts as a nurse without any pain!
If the physical therapy treatment you are receiving does not get feeling better within 1 or 2 weeks, find something that works!
More
Quick Answers Are Never a Guarantee

We live in a culture that seeks immediate results and quick answers to solutions. Most of the time, unfortunately, we also want what requires the least amount of effort on our part. In the medical community, this boils down to people deciding to have surgery to fix the problem. Unfortunately, surgery is never a guarantee. Time and time again I treat patients here at Nick Rinard Physical Therapy who were advised to have surgery and, after the procedure was performed, their pain remained. This happens because of both the general public and medical practitioners’ lack of understanding about how the body moves and heals. Recently, there was a man referred to our Portland airport (PDX) clinic by his friend for knee pain. He was scheduled to have knee surgery the next week, but wanted to have a second opinion. My colleague diagnosed him with a very simple problem: knee capsulosis, and he was reporting decreased pain and improved range of motion by his 2nd visit. He cancelled his surgery and is expected to have a great outcome with conservative care.
Regimented Exercise Can Decrease Knee Pain without Surgery
I recently came across a study that found simple regimented exercise routine focusing on quadriceps strengthening and cardiovascular endurance decreases knee pain associated with osteoarthritis. What a great concept: exercise can decrease pain and improve function and avoid surgery! The authors of the study concluded: “Optimal exercise programs for knee OA should have one aim and focus on improving aerobic capacity, quadriceps muscle strength, or lower extremity performance,” the authors concluded. “For best results, the program should be supervised and carried out three times a week. Such programs have a similar effect regardless of patient characteristics, including radiographic severity and baseline pain.”
Physical Inactivity is THE Major Public Health Problem of the 21st Century
I came across a quote that really resonates with these findings: “…most medical schools only allocate a perfunctory hour to the fact that physical activity is medicine. This is a major failing of medical education when physical inactivity is the major public health problem of the 21st century.”
Resources
Meta-analysis: Quadriceps exercise best reduces knee OA pain:
http://news.todayinpt.com/article/20140329/TODAYINPT04/140328005&SearchID=73533945353381?utm_content=sf25084815&utm_medium=spredfast&utm_source=facebook&utm_campaign=social2013&sf25084815=1
Accessed on May 1st, 2014
Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. K M Khan, A Scott. Br J Sports Med 2009;43:247-252
More
Recently, I have had 3 physical therapy patients in the clinic with a complicated clinical presentation. All 3 patients have a different cluster of symptoms and impairments. What they each have in common is that they have upper extremity symptoms that are not of cervical spine (radiculopathy) origin. Instead, their pathology is a result of tight chest and neck musculature, compressing the bundle of nerves that control the movement and sensation of the arm. Clinically, this is known as Thoracic Outlet Syndrome, or, TOS.
What is Thoracic Outlet Syndrome?
- Compression of the artery, vein and/or nerves that pass through the thoracic outlet.
- There are 3 possible locations for the compression to occur:
- In between your scalene (neck muscles)
- In between the clavicle and first rib
- Under the peck minor (chest muscle)
| The most common compression is of the nerves. This results in vague pain of the arm as well as various sensations: itchy, hot, cold, pins and needles, etc.It may be painful to the touch for any of the muscles involved with the compression.
Poor posture as well as decreased flexibility of the thoracic spine are also associated with TOS.
Rarely, an extra rib (cervical rib) is the cause. |
 |
Physical Therapy Treatment for TOS
- Physical therapy is the first line of treatment for Thoracic Outlet Syndrome (TOS).
- A therapist will teach you how to stretch what needs to be lengthened as well as how to strengthen muscles that will improve posture.
- Physical therapists also have manual techniques to help you progress your treatment
- Most people diagnosed with TOS have a good prognosis and will have complete resolution of symptoms with conservative treatment only.
More
Lateral epicondylitis, more commonly known as “tennis elbow,” is a pathology that is familiar to physical therapists and the general public. What is lesser known is “pseudo tennis elbow,” a mechanical problem with a very simple solution! Unfortunately, therapists whom are not familiar with the utilization of mechanical diagnosis may unknowingly miss this common elbow derangement. As a therapist practicing the McKenzie method of mechanical diagnosis, I have diagnosed BOTH of my current elbow pain patients as derangements (or pseudo tennis elbow).
SYMPTOMS
Portland area patient presented to physical therapy with intermittent right elbow pain, worsening over the last 3 months. Patient reported difficulty with gripping, lifting, carrying and global limited function of the right arm. Patient described symptoms as “variable” meaning he could perform a task that produced his elbow pain. Then, perform the same task or movement again without experiencing any pain at all! This variability of pain is the hallmark of a derangement and should not be misdiagnosed as a tendonitis (also called tendinitis), which would indicate inflammation (in which case pain would be constant). Patient rated worst elbow pain as a 6/10.
THERAPIST’S EVALUATION AND FINDINGS
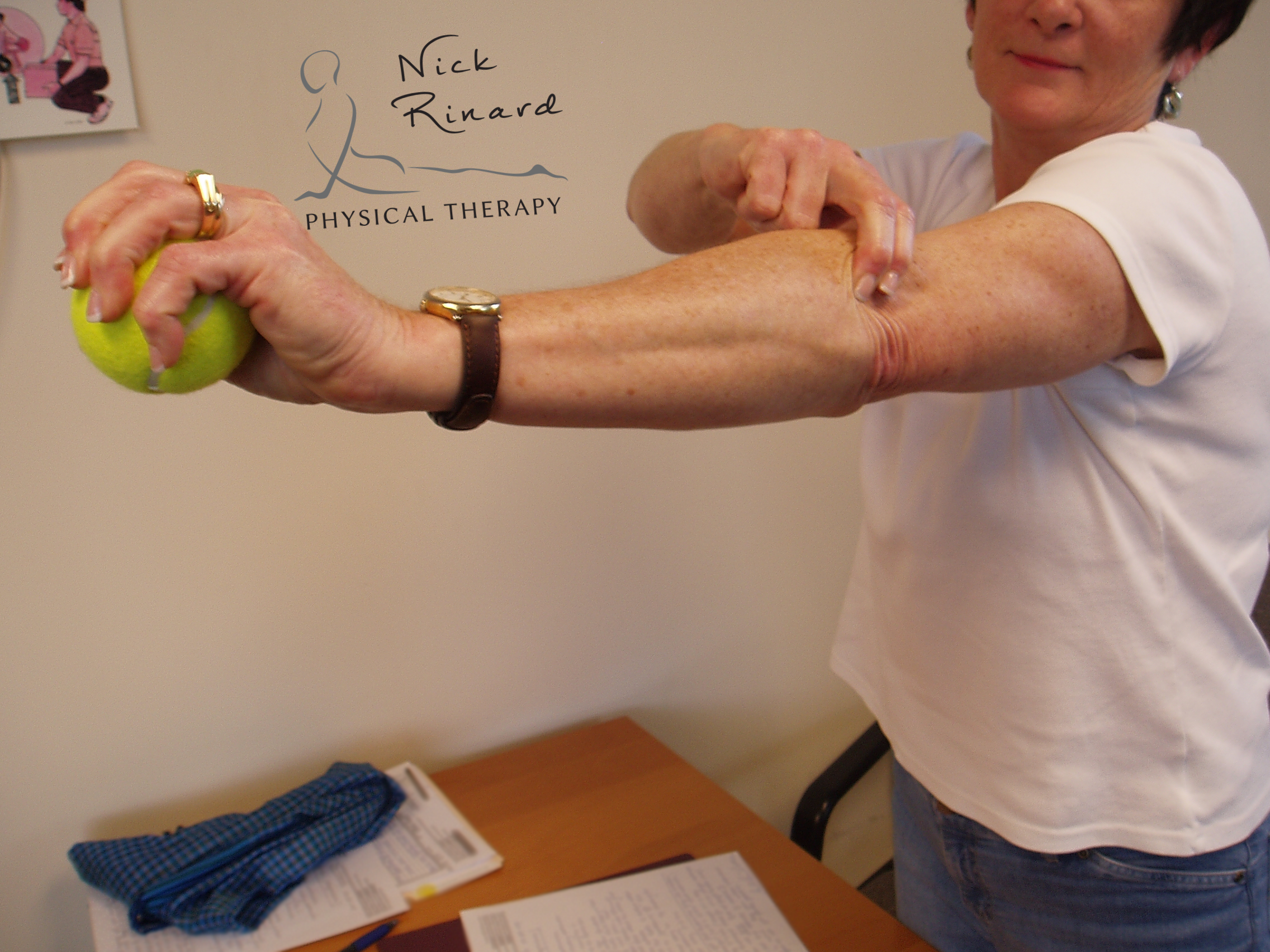
 Objective findings included pain with passive elbow flexion and extension as well as pain with active wrist extension and with gripping a tennis ball. Because of my experience as a mechanical therapist, I am familiar with a technique called a mobilization with movement (MWM), developed by Brian Mulligan (a colleague of Robin McKenzie). The mobilization provides a lateral force over the ulna at the elbow joint. While the patient applied this force, he was able to grip the tennis ball PAIN FREE! This same technique was applied for other painful baselines and achieved the same results of ABOLITION OF ALL PAIN! This ability to turn symptoms off with a mobilization indicates an elbow derangement and the MWM is used as the treatment strategy.
Objective findings included pain with passive elbow flexion and extension as well as pain with active wrist extension and with gripping a tennis ball. Because of my experience as a mechanical therapist, I am familiar with a technique called a mobilization with movement (MWM), developed by Brian Mulligan (a colleague of Robin McKenzie). The mobilization provides a lateral force over the ulna at the elbow joint. While the patient applied this force, he was able to grip the tennis ball PAIN FREE! This same technique was applied for other painful baselines and achieved the same results of ABOLITION OF ALL PAIN! This ability to turn symptoms off with a mobilization indicates an elbow derangement and the MWM is used as the treatment strategy.
PATIENT HOMEWORK and OUTCOMES
The patient was asked to perform the MWM utilizing the lateral glide while gripping a tennis ball to be performed 10-20 times every hour. The theory is that this mobilization is re-positioning the joint in order for it to articulate correctly, resulting in improved range of motion and strength after. The patient returned to the clinic the next day with reports of at least 25% improvement! Objective findings were retested and nearly all baselines had improved in less than 24 hours! The patient returned 1 week later and reported an 85% overall improvement with symptoms.
GET YOURSELF EVALUATED
Don’t be misdiagnosed! Straightforward pathologies which require one exercise to treat are commonly missed with standard treatment. This results in extra physical therapy visits, and more of your time and money. It is worth your time to see if your pain has a MECHANICAL component, otherwise a simple solution may otherwise be missed.
If you are experiencing elbow pain and are living in the Portland/Vancouver metro area, get the best results by calling us today at 503-244-6232 to schedule a physical therapy evaluation.
More
I recently had a follow up appointment with a patient of mine. “Sam” came to our clinic after having failed attempts of treatment from standard Physical Therapy and chiropractic care. His past physical therapist had given him generalized stretching with little to no benefit, and by the time I evaluated him, Sam admitted that, “(he) was not impressed with his therapy treatment.” He had heard about Nick Rinard Physical Therapy, and he was hoping to get the results he desired with us.
During his initial evaluation, Sam presented with limited, painful movements in several motions of the shoulder. The most painful motion was the motion of putting the arm behind him (like he was going to scratch in between his shoulder blades). Incidentally, this was also the motion which initially caused his pain three months ago.
 I had Sam passively stretch into the painful motion. This was not a random decision. It was a clinical decision based off of his baselines and has been clearly documented and researched by the works of Mark Laslett. As Sam repeated this movement, the pain dissipated and all of his baselines improved. Sam continued to perform this exercise until his next visit, at which, he reported 95% improvement.
I had Sam passively stretch into the painful motion. This was not a random decision. It was a clinical decision based off of his baselines and has been clearly documented and researched by the works of Mark Laslett. As Sam repeated this movement, the pain dissipated and all of his baselines improved. Sam continued to perform this exercise until his next visit, at which, he reported 95% improvement.
Sometimes the exercise required to fix the mechanical problem is counterintuitive (moving into the pain). A trained mechanical therapist is able to recognize these pain patterns and can make a clinical decision as to what exercise should be performed and interpret the results.
More