Don’t take our word for it….
“Had great results with previous issues.
Decided to come back to address some chronic issues from my past.
I’m actually able to engage my right lower shoulder blade.
A long way to go, but am on my way to being able to strength train again.”
Daniel
More
By Nick Rinard MPT, Cert MDT
09 Jun, 2014
Clinical Case of the Week
abduction, chronic, dosed loading, dysfunction, falling, flexion, remodeling, shoulder pain, suprapinatus
 Patient is a 60 y/o male “Mike” with chronic shoulder pain. Mike’s symptoms started in 1994 after falling onto his left shoulder. Overall, his symptoms had been unchanging and severely affecting his job. He has had previous physical therapy and massage therapy to no avail. He was severely limited with lifting, carrying and working out.
Patient is a 60 y/o male “Mike” with chronic shoulder pain. Mike’s symptoms started in 1994 after falling onto his left shoulder. Overall, his symptoms had been unchanging and severely affecting his job. He has had previous physical therapy and massage therapy to no avail. He was severely limited with lifting, carrying and working out.
During his initial evaluation, it was found that Mike had painful, limited range of all shoulder movements with the exception of lateral rotation. He also had weak/painful resisted tests of shoulder abduction, medial rotation and flexion. His most limited impairment was painful, weak abduction.
It was determined that Mike had chronic dysfunction of the supraspinatus muscle tendon (one of the rotator cuff muscles). Because of the anatomical position of this tendon, it is the most commonly injured and torn of the rotator cuff. Mike began remodeling his tendon with targeted, dosed loading. By the next visit, he was strong, in less pain and had improved range of motion.
Mike continued his remodeling exercises for the next 4 weeks. By his 6th visit to our Portland clinic he had virtually no pain and was no longer limited with his work or life from his shoulder pain. Mike is a classic example of how conservative treatment that targets the root of the problem results in fast, effective results!
Don’t wait 20 years to have your simple problem solved. Have a mechanical evaluation at Nick Rinard Physical Therapy today!
More
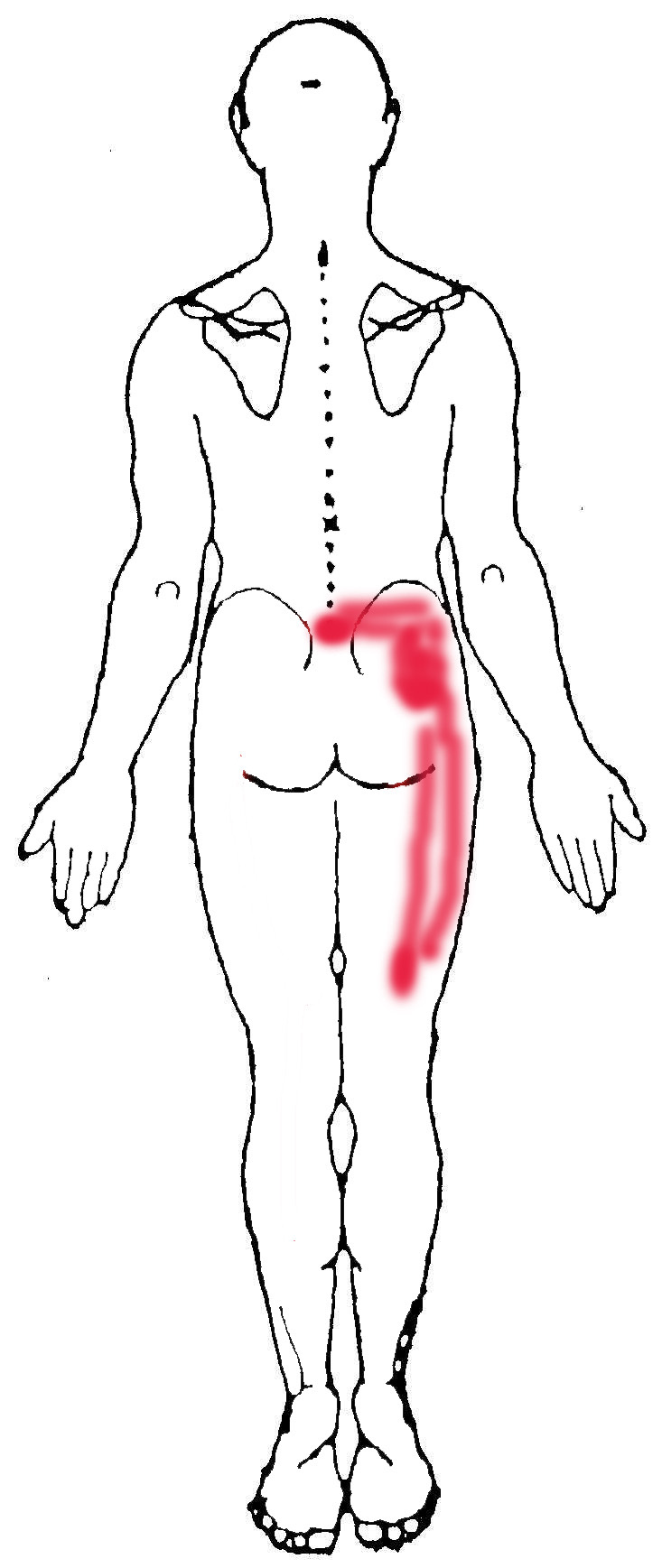
 The case study I would like to share with you today is only the second hip derangement of this type that I have seen in 18 years of practice. “Jim” was a 55 year old male who presented with right hip pain that started for no apparent reason 5-6 months prior to coming to physical therapy. He said the pain was provoked only when he was walking, but it occurred consistently at a distance of about 50 to 100 yards. Often it was so painful he could not continue walking. Jim figured out that changing his right foot position enabled him to walk a little further, albeit slowly, and then he could resume normal walking for another 50 yards or so. He would change the foot position by stepping partway onto a curb or raised ground such that the outer edge of his foot was tilted up (eversion, as we therapists call it), and then he would angle his right knee inwardly. That was the only way he had found to improve walking, but the hip just would not stay better.
The case study I would like to share with you today is only the second hip derangement of this type that I have seen in 18 years of practice. “Jim” was a 55 year old male who presented with right hip pain that started for no apparent reason 5-6 months prior to coming to physical therapy. He said the pain was provoked only when he was walking, but it occurred consistently at a distance of about 50 to 100 yards. Often it was so painful he could not continue walking. Jim figured out that changing his right foot position enabled him to walk a little further, albeit slowly, and then he could resume normal walking for another 50 yards or so. He would change the foot position by stepping partway onto a curb or raised ground such that the outer edge of his foot was tilted up (eversion, as we therapists call it), and then he would angle his right knee inwardly. That was the only way he had found to improve walking, but the hip just would not stay better.
In desperation, Jim said he had looked online and tried numerous “hip exercises” without any relief. He consulted his doctor, who recommended MDT, which we do here at Nick Rinard Physical Therapy.
Assessment
The mechanical assessment was positive for only two findings: limited and painful hip motion into flexion (folding the knee to chest), and weak and painful testing of hamstring resistance. The protocol for ruling out a joint derangement is to repeat motions to determine if the baselines change. The question is which motion to repeat. One can move either into the most painful direction, go the opposite direction, or check rotations. I chose to go into the most painful direction, in this case, flexion. But before testing I wanted to establish how far Jim could walk in the clinic before his pain started. By the time he walked one length of the hallway and back, he reported pain. I then instructed Jim to bend his knee to chest (compressing the groin) repeatedly and after 20 to 30 times. It produced his familiar pain initially, then the pain abolished and his motion increased. I tested walking after that and Jim said there was no pain even after walking 3 lengths up and back through the hallway! I gave Jim his exercises and scheduled him for 2 days later.
Progress
When Jim returned he reported that he could walk longer distances without the pain starting, however, he still got to the point where he had to modify his foot position in order to continue. I knew we were on the right track, and the next step in treating a joint derangement is to progress forces. I did this manually by applying over-pressure, and instructed Jim to do it in standing by folding his chest down to his knee with it supported on a bench or chair. By the next visit, Jim reported that this had worked very well and he had not experienced any pain at all! So, the derangement was reduced and I needed to wean him off the home exercises to see if it would return or not. I gave him the weaning program and asked to see him back in 2 weeks.
Pain Free
After 2 weeks, Jim came back reporting that he had been able to walk unlimited distances! He resumed walking his dog, going on walks for exercise, and walking wherever, and whenever he wanted. He reported his longest walk lasted 4.5 hours. He said there was no return of the original hip pain from which he had suffered for months. However, on his last two walks, he had started noticing a new hip pain, this time in the front, not on the sides. I re-checked his baselines and neither flexion motion nor resisted hamstrings were painful. That meant it could not be a re-derangement. Resisted hip flexion was painful, and that was new. I concluded that his sudden ability to walk pain-free resulted in his over-doing it. Jim had increased walking too fast and gotten a minor tendonitis. That was easy to treat, and by his next visit, Jim was pain-free again and able to progress walking, though this time more gradually, which was safer.
Successful Treatment
Jim’s hip treatment was obviously a success. It took only 4 visits. This hip derangement was unique because the direction that reduced it (flexion); I have only seen one other hip derangement require flexion to reduce it. The fact that Jim resumed normal activity too fast is typical of reduced derangements – the patient feels so good that they over do it. Luckily in Jim’s case, we found the new problem and fixed it just as fast as we found and fixed his chronic hip pain.
More