“I had continual cervical pain related to a motor vehicle accident.
The pain affected my ability to sleep, read, work, drive, watch tv, and turn my head without pain.
Now, I can do all the above activities and recreational sport activities.”
John
More
What a year to review!
Are you having shoulder pain?
“After surgery on my left shoulder I needed a ton of help regaining movement & strength.
I can do pretty much everything that I could do before my injury now – which I didn’t expect would be possible so THANK YOU SO MUCH!“
Amanda
Are you having low back pain?
“I came after severe back pain. I was not able to bend over, walk for extended time, or sit without pain.
Right away I had better results from doing the exercises I was shown then I had ever had with my previous therapist.
I feel like we went at a good pace and throughout my treatment I have been able to increase my overall activity and quality of life.
I have been given the knowledge and tools I need to manage my pain on my own and my back pain has greatly improved!”
Danielle
Are you having knee pain?
“I chose to come here because I read such great reviews.
After reading just a few, I knew this was the place where I needed to be.
I came for my knee, but after completing physical therapy for it, it feel like a lot more than just my knee has improved.
I have better knowledge of mind and body connection, much better balance, and my whole body is stronger overall.
This office has great energy and everyone who needs physical therapy should come here! ”
Ronnie
Failed back surgery?
“I was recommended to investigate the McKenzie Method for my recover, especially as my pain had greatly increased and did not seem to be improving.
The PT folks I was seeing at that time recommend that I check you all out as practitioners of this method. Although eventually we all concluded that a follow up surgery to replace my disk is necessary.
I have much more confidence that I will be able to live a life pain-free, or much reduced.
At the moment I can stand straighter than before, can drives for a short distance if necessary, and better manage my own pain w/o opioids.”
Brian
Let your New Year resolution be one of these testimonials.
Rid yourself of pain and get back to pre-injury/surgery levels!
More
So your New Year’s Resolution is to finally get moving with an exercise program. That’s excellent! You make it to the gym and hurl yourself into a routine full of good intentions. But, your body may have other ideas.. your knees are screaming, your back is hurting, and your shoulders are nagging you. At Nick Rinard Physical Therapy, we are here to help you quiet those aching joints and become successful with your new exercise routine! Less than 52% of Americans get adequate weekly aerobic exercise (https://www.cdc.gov/nchs/fastats/exercise.htm); we are here to help you beat that statistic!

More
By Megan Plante, DPT
07 Apr, 2016
Physical Therapy Tips
age, aging, balance, challenge, dynamic, exercises, general, knowledge, Physical Therapy, practice, static
It is general knowledge that, as we age, our sensory systems start to decline. This includes sight, smell, temperature regulation and balance mechanisms. It’s important to have good balance because if it declines, you are at a higher risk for falling. And falling, results in injuries that can greatly affect your life.
Exercises that Challenge your Balance
What many people don’t know, is that you can work on making your balance stronger, just like you do a muscle: by exercising it! What physical therapy aims to do, is find exercises that challenge your balance system, so that your body must learn to adapt to certain situations and re-train itself on what to do.
Static and Dynamic Exercises
Physical Therapists can provide both static and dynamic exercises for you, depending on what is most challenging. Exercises can be very simple and integrated during daily routines- like balancing on one leg while brushing your teeth.
If you are having trouble with your balance, come in to Nick Rinard Physical Therapy and have an assessment by a physical therapist! 503-244-6232
More
By Megan Plante, DPT
12 Jun, 2014
Clinical Case of the Week
exercises, inactivity, Knee pain, MDT, medical education, Nick Rinard, OA pain, Portland Oregon, quadricepts, quick answers
Quick Answers Are Never a Guarantee
We live in a culture that seeks immediate results and quick answers to solutions. Most of the time, unfortunately, we also want what requires the least amount of effort on our part. In the medical community, this boils down to people deciding to have surgery to fix the problem. Unfortunately, surgery is never a guarantee. Time and time again I treat patients here at Nick Rinard Physical Therapy who were advised to have surgery and, after the procedure was performed, their pain remained. This happens because of both the general public and medical practitioners’ lack of understanding about how the body moves and heals. Recently, there was a man referred to our Portland airport (PDX) clinic by his friend for knee pain. He was scheduled to have knee surgery the next week, but wanted to have a second opinion. My colleague diagnosed him with a very simple problem: knee capsulosis, and he was reporting decreased pain and improved range of motion by his 2nd visit. He cancelled his surgery and is expected to have a great outcome with conservative care.
Regimented Exercise Can Decrease Knee Pain without Surgery
I recently came across a study that found simple regimented exercise routine focusing on quadriceps strengthening and cardiovascular endurance decreases knee pain associated with osteoarthritis. What a great concept: exercise can decrease pain and improve function and avoid surgery! The authors of the study concluded: “Optimal exercise programs for knee OA should have one aim and focus on improving aerobic capacity, quadriceps muscle strength, or lower extremity performance,” the authors concluded. “For best results, the program should be supervised and carried out three times a week. Such programs have a similar effect regardless of patient characteristics, including radiographic severity and baseline pain.”
Physical Inactivity is THE Major Public Health Problem of the 21st Century
I came across a quote that really resonates with these findings: “…most medical schools only allocate a perfunctory hour to the fact that physical activity is medicine. This is a major failing of medical education when physical inactivity is the major public health problem of the 21st century.”
Resources
Meta-analysis: Quadriceps exercise best reduces knee OA pain:
http://news.todayinpt.com/article/20140329/TODAYINPT04/140328005&SearchID=73533945353381?utm_content=sf25084815&utm_medium=spredfast&utm_source=facebook&utm_campaign=social2013&sf25084815=1
Accessed on May 1st, 2014
Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. K M Khan, A Scott. Br J Sports Med 2009;43:247-252
More
LOW BACK PAIN—What you should do while waiting for your first physical therapy appointment…
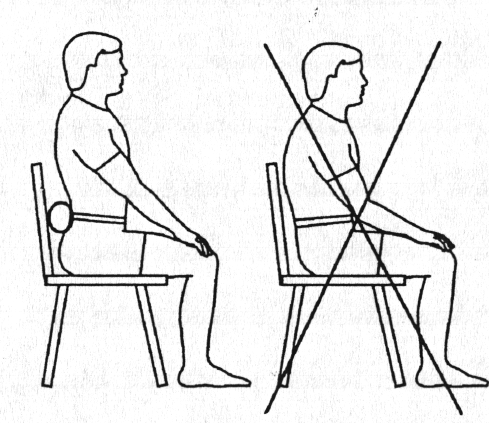
SITTING:
 Sit as little as possible. Standing or lying down are preferable to sitting when in acute low back pain. If you must sit, sit only in a straight backed chair with good posture. Avoid couches or soft chairs. Use a towel roll to support the natural curve of your spine.
Sit as little as possible. Standing or lying down are preferable to sitting when in acute low back pain. If you must sit, sit only in a straight backed chair with good posture. Avoid couches or soft chairs. Use a towel roll to support the natural curve of your spine.
BENDING:
Do not bend forwards as in touching your toes when in acute low back pain—even if it feels like you are doing good by “stretching” the muscles of the low back. Rather than reaching down to get things, squat down using the legs and keep the back absolutely straight.
LYING:
Try to lie more on your stomach rather than on your back. Avoid the temptation to lie on your back with the head and knees propped up—this just rounds the back more and places inappropriate stress on injured structures.

EXERCISES:
You should stay normally active–in other words try not to stay in bed for long periods. Move around, take walk if you can. Do not do the knees to chest exercise you may have learned before. This is an advanced exercise and usually not appropriate for acute conditions. It is better in most cases to lie on your stomach and work towards supporting yourself on the elbows.
 |
 |
| NO! |
YES! |
More
 The case study I would like to share with you today is only the second hip derangement of this type that I have seen in 18 years of practice. “Jim” was a 55 year old male who presented with right hip pain that started for no apparent reason 5-6 months prior to coming to physical therapy. He said the pain was provoked only when he was walking, but it occurred consistently at a distance of about 50 to 100 yards. Often it was so painful he could not continue walking. Jim figured out that changing his right foot position enabled him to walk a little further, albeit slowly, and then he could resume normal walking for another 50 yards or so. He would change the foot position by stepping partway onto a curb or raised ground such that the outer edge of his foot was tilted up (eversion, as we therapists call it), and then he would angle his right knee inwardly. That was the only way he had found to improve walking, but the hip just would not stay better.
The case study I would like to share with you today is only the second hip derangement of this type that I have seen in 18 years of practice. “Jim” was a 55 year old male who presented with right hip pain that started for no apparent reason 5-6 months prior to coming to physical therapy. He said the pain was provoked only when he was walking, but it occurred consistently at a distance of about 50 to 100 yards. Often it was so painful he could not continue walking. Jim figured out that changing his right foot position enabled him to walk a little further, albeit slowly, and then he could resume normal walking for another 50 yards or so. He would change the foot position by stepping partway onto a curb or raised ground such that the outer edge of his foot was tilted up (eversion, as we therapists call it), and then he would angle his right knee inwardly. That was the only way he had found to improve walking, but the hip just would not stay better.
In desperation, Jim said he had looked online and tried numerous “hip exercises” without any relief. He consulted his doctor, who recommended MDT, which we do here at Nick Rinard Physical Therapy.
Assessment
The mechanical assessment was positive for only two findings: limited and painful hip motion into flexion (folding the knee to chest), and weak and painful testing of hamstring resistance. The protocol for ruling out a joint derangement is to repeat motions to determine if the baselines change. The question is which motion to repeat. One can move either into the most painful direction, go the opposite direction, or check rotations. I chose to go into the most painful direction, in this case, flexion. But before testing I wanted to establish how far Jim could walk in the clinic before his pain started. By the time he walked one length of the hallway and back, he reported pain. I then instructed Jim to bend his knee to chest (compressing the groin) repeatedly and after 20 to 30 times. It produced his familiar pain initially, then the pain abolished and his motion increased. I tested walking after that and Jim said there was no pain even after walking 3 lengths up and back through the hallway! I gave Jim his exercises and scheduled him for 2 days later.
Progress
When Jim returned he reported that he could walk longer distances without the pain starting, however, he still got to the point where he had to modify his foot position in order to continue. I knew we were on the right track, and the next step in treating a joint derangement is to progress forces. I did this manually by applying over-pressure, and instructed Jim to do it in standing by folding his chest down to his knee with it supported on a bench or chair. By the next visit, Jim reported that this had worked very well and he had not experienced any pain at all! So, the derangement was reduced and I needed to wean him off the home exercises to see if it would return or not. I gave him the weaning program and asked to see him back in 2 weeks.
Pain Free
After 2 weeks, Jim came back reporting that he had been able to walk unlimited distances! He resumed walking his dog, going on walks for exercise, and walking wherever, and whenever he wanted. He reported his longest walk lasted 4.5 hours. He said there was no return of the original hip pain from which he had suffered for months. However, on his last two walks, he had started noticing a new hip pain, this time in the front, not on the sides. I re-checked his baselines and neither flexion motion nor resisted hamstrings were painful. That meant it could not be a re-derangement. Resisted hip flexion was painful, and that was new. I concluded that his sudden ability to walk pain-free resulted in his over-doing it. Jim had increased walking too fast and gotten a minor tendonitis. That was easy to treat, and by his next visit, Jim was pain-free again and able to progress walking, though this time more gradually, which was safer.
Successful Treatment
Jim’s hip treatment was obviously a success. It took only 4 visits. This hip derangement was unique because the direction that reduced it (flexion); I have only seen one other hip derangement require flexion to reduce it. The fact that Jim resumed normal activity too fast is typical of reduced derangements – the patient feels so good that they over do it. Luckily in Jim’s case, we found the new problem and fixed it just as fast as we found and fixed his chronic hip pain.
More